
Improving Healthcare for All
Accessible healthcare should be a human right, not a luxury.
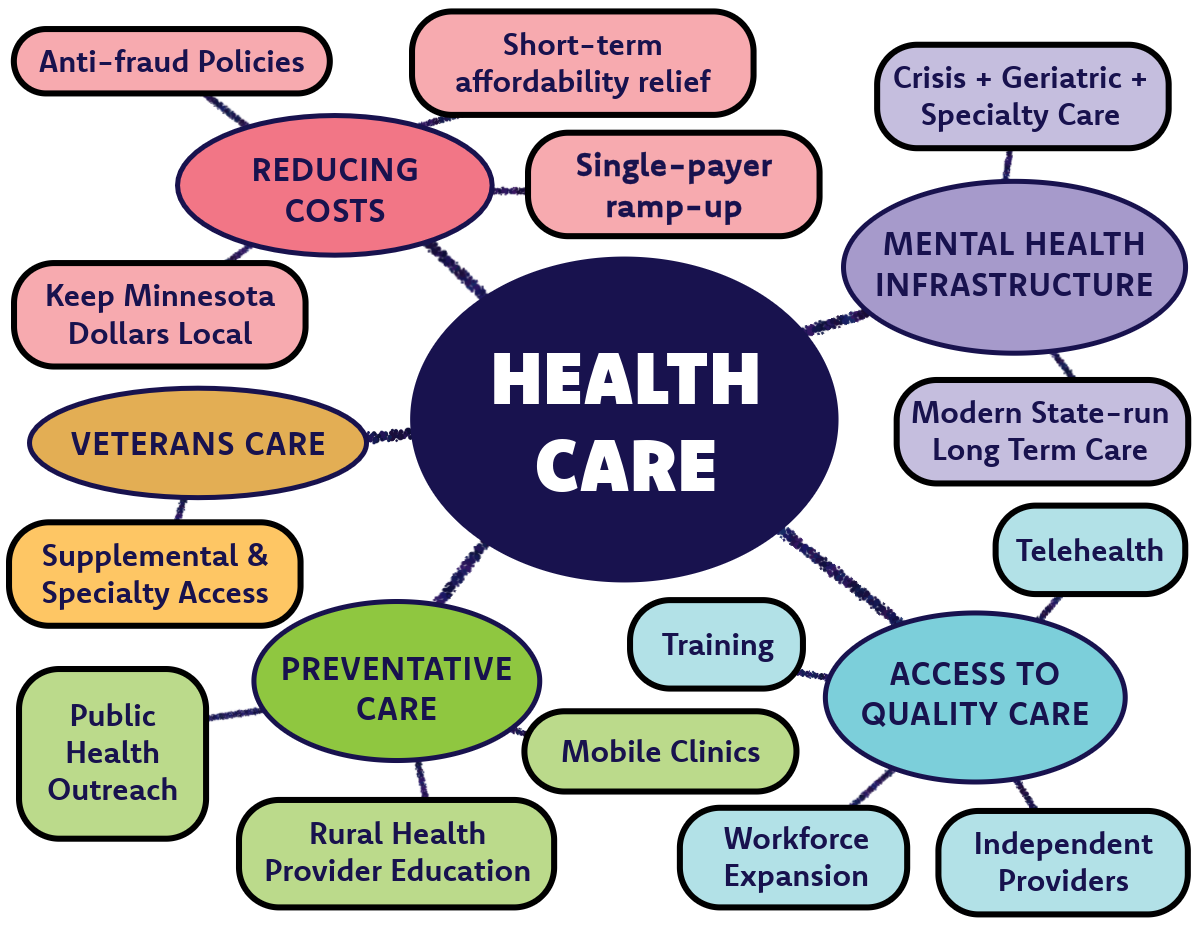
Expand Accessibility to Quality Care: Healthcare in rural Minnesota can be a bit of a struggle. Many rural Minnesotans face challenges to receiving good care because of long travel times or a lack of available services. Some contributing factors are provider shortages, long wait times for specialists, or even rural hospital and clinics are closures or at risk closures across greater Minnesota (note: these hospital systems often cite financial distress and reimbursements issues and these closures drives up costs at nearby "surviving" hospital systems; Mille Lacs Health System, Hennepin Healthcare [one of only five level 1 trauma hospitals in MN], Mayo Clinic, Fairview Range Medical Center [at risk]). I support policies that expand telehealth services, which will help people across greater Minnesota connect with specialists and primary care providers. This expansion will help improve prompt care and reduce costs associated with travel-related expenses (including time off work). Similarly, I will also advocate for rural healthcare workforce incentives to attract healthcare providers to traditionally underserved rural areas, including expanded student loan forgiveness and rural Minnesota physician scholarships. Additionally, I support exploring options that make it easier for independent practitioners to open and maintain community‑based practices outside the control of large hospital systems. When we strengthening pathways for independent providers, we will increase competition (which could drive down prices), expand access to underserved areas, and keeps care local. Let’s be honest: Minnesota isn’t running out of smart, capable people. We’re running out of ways to get them into healthcare. Our state is full of individuals with advanced degrees that left the workforce to raise children or care for family members, as well as mid‑career adults who would jump into healthcare tomorrow if the path weren’t so rigid and expensive. I know... I am one of them. I support creating scholarships and training programs for people with advanced health-related degrees who want to transition into healthcare practice, and for Minnesotans re‑entering the workforce after caregiving. We need to eliminate barriers to training. Rest assured, opening more doors will not lower the quality of care, but it will bring more well‑trained and motivated practitioners into communities that could really use them.
Improve Mental Health Resources: Beginning in the 1960s and throughout the 1990s, states across the country closed their public psychiatric hospitals as part of a nationwide movement known as deinstitutionalization. The idea was that new medications and community‑based care would replace long‑term state facilities. Minnesota embraced this shift more aggressively than most states and closed nearly all of its state hospitals under the premise that private and nonprofit systems would pick up the care. Short story: They didn’t, and rural communities have been living with the consequences ever since. People wait months for appointments, drive hours for basic services, skip care altogether, or end up in emergency rooms and county jails because the public backbone that once provided long‑term treatment no longer exists. I support rebuilding modern and humane state‑run long‑term care facilities that meet today’s needs, including: psychiatric stabilization, extended mental‑health treatment, crisis services, geriatric and memory care, rehabilitation, addiction treatment, and supplementary services for veterans. These are essential services the private market has never delivered at the scale rural Minnesota needs. Rebuilding this system also connects directly to the workforce solutions outlined in "Expand Accessibility to Quality Care" with scholarships, paid clinical training, and alternative pathways for those with a passion for mental health. Rural Minnesotans deserve a mental health system that actually exists, and restoring the public infrastructure we dismantled is the only way to get there.
Reducing Costs: Medical debt is the leading cause of bankruptcy in the United States and approximately 2% of Minnesota households have medical debt in collections. Healthcare has been made to be expensive, especially insurance. When it comes to breaking down where every dollar of health insurance goes, >20% go to profits (~3%; but this is questionably low) and administrative costs (18%), including paying the bloated salary of insurance executives, marketing, call-center operations, claims processing, and even paying the non-medical personnel that are in charge of of determining preauthorizations or deny medical decision coverage (read about the US Senate Permanent Subcommittee on Investigations report on prior authorizations, or follow the case of Estate of Gene B. Lokken Vs. UnitedHealth Group, Case No. 23-cv-3514 (JRT/SGE) for a class action lawsuit concerning the use of AI in medical decisions). The current system sends too much of our money for non-medical purposes while providing little in return. I support the transition to a single-payer healthcare system, which will decrease costs by eliminating the middle man and administrative waste, all while creating a state-run insurance program with stable, good-paying jobs right here in Minnesota. Experience has shown us that piecemeal or phased approaches that are market-based do not work to bring prices down for the long-term (see the Massachusetts Model for Healthcare (Romneycare, 2006) and the Affordable Care Act). Partial reforms leave gaps, delays, and cost overruns, while subsidizing insurance companies. The winner is definitely not the taxpayer. Minnesota needs a single-payer system that is ramped up deliberately and then rolled out statewide so every Minnesotan has access to healthcare without being tied to employer‑based benefits. And fraud? Well, we get ahead of fraud by supporting policies that demand accountability and increase penalties against practitioners and systems that engage in fraudulent activities or falsifications (e.g. double billing, inflated charges).While building toward the long-term solution of single-payer healthcare, I support short-term solutions for reducing costs, like expanded prescription assistance programs, increased MinnesotaCare access for people with serious illnesses, and revisiting the sliding-scale subsidy system tied to income to make healthcare more affordable. These short-term efforts will help Minnesotas now, while we prepare for a more efficient and equitable healthcare system that ensures Minnesota healthcare dollars are used for healthcare.
Improved Preventative Care: As a biomedical scientist, I cannot underscore this enough: High quality prevention and intervention will always be more cost-effective than a cure. Preventative care keeps people healthier and saves money, but it only works if Minnesotans can access services that they trust. I support education policies for health practitioners that prepare them for a career in rural medicine, including training for cultural competency, bedside manner, and handling misinformation. Additionally, I support expanding preventative care across rural Minnesota through mobile clinics that can provide screenings, chronic‑disease management, and mobile vaccination services to rural, underserved communities. Preventative care also depends on trustworthy information, and too many Minnesotans have been left to sort through a half‑truths and misinformation. We can and must combat healthcare skepticism with facts, which is why I support public health education outreach that is built on transparency, including citations to primary literature, layman summaries, and full disclosure and scrutiny of any conflicts of interest. Together with improved healthcare accessibility and reduced costs (see above), preventative care will become accessible, affordable, and credible. Minnesotans will stay healthy without waiting for a healthcare crisis.
Improved Accessibility to Healthcare for Veterans: Veterans in rural Minnesota can face some steep barriers to care, with long travel distances and staffing shortages that can make some appointments difficult. Specialty care including dental, mental health, emergency care, ophthalmology (eyes and visual system), orthopedics, urology (urinary), and others, is lacking in the Brainerd Lakes area and across much of rural Minnesota. I support supplementing VA care through the healthcare reforms already highlighted in my platform, including: modern state‑run long‑term care facilities that include psychiatric, addiction, rehabilitation, geriatric, and memory‑care services; expanded telehealth; mobile preventative‑care and vaccination clinics; and an expanded healthcare workforce that increases access to mental‑health providers and specialists across greater Minnesota. These policies apply to all Minnesotans, but they directly benefit veterans by shortening wait times, expanding specialty access, and ensuring they can receive timely, comprehensive care along with the benefits they’ve earned through the VA.
Go and learn something about the state of healthcare in rural Minnesota: Rural Health Care in Minnesota: Data Highlights by the Minnesota Department of Health